Julia Kelley
Poor access to clean water and underdeveloped facilities has led Nigeria to face a decades-long, deadly battle against cholera.

Access to Safe Water in Nigeria. EU Civil Protection and Humanitarian Aid. CC BY-NC-ND 2.0.
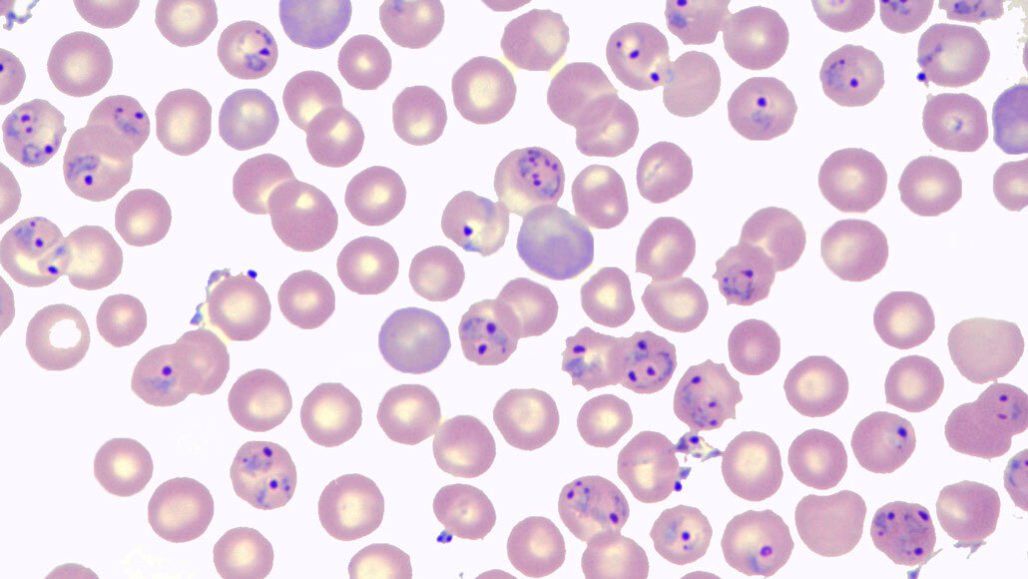
For decades, Nigeria has faced major cholera outbreaks throughout the country, posing a serious threat to public health. The disease, an acute diarrheal infection caused by ingesting food or water contaminated with the bacterium Vibrio cholerae, is a major indication of inequity, as well as a lack of social and economic development in the areas where it forms. Since 1972, cholera has plagued Nigeria in intermittent outbreaks that have claimed thousands of lives, the worst being in 1991, with a high of 59,478 reported cases and 7,654 deaths. Despite numerous attempts by the World Health Organization, the Nigeria Center for Disease Control and the Borno State Ministry of Health to provide support through free cholera vaccines and implement prevention and preparedness, the country continues to fight against large, destructive outbreaks.
Many factors make Nigeria especially prone to these widespread epidemics, including a lack of access to safe drinking water, a lack of infrastructure necessary for water supply and waste disposal and a lack of health facilities. Particularly in smaller communities and remote villages, sourcing clean water is a challenge that leads residents to dig their own wells. Moreover, during the dry season, these wells dry up and leave individuals only with the more hazardous alternative of shallow streams. Poor weather conditions worsen this significant obstacle to clean water and sanitation. Flooding, for example, increases food insecurity by destroying farmland, creating economic loss, demolishing sanitation facilities and contaminating sources of clean water. Several financial issues, including poor investment, funding allocation and low human capital, in conjunction with already deficient infrastructure and low community participation, also contribute to a lack of secure water infrastructure. Not only does this make for a higher potential of infection, but Nigera’s healthcare infrastructure is also underdeveloped, lacking the medical facilities and supplies necessary to treat those infected with cholera. Limited medical equipment and supplies, as well as a lack of internet connectivity, make it extremely difficult to heal patients and facilitate important reporting of cholera data.
These issues remain significant and continue to threaten the lives of Nigeria’s citizens. This is exemplified by the country’s most recent outbreak in 2024, which saw about 11,000 recorded cases and 359 deaths in October that year. Intense rains throughout the year led to widespread floods and dam breaks across Nigeria, weakening water infrastructure, destroying farmland and leaving many homeless in damaged areas, overall causing a large part of the country to be vulnerable to diseases like cholera. This most recent epidemic was met with policy and prevention program recommendations in the hope of impeding future spreads, the most critical of which being Water, Sanitation and Hygiene services. These accelerate and sustain access to safe water, sanitation services and good hygiene practices, all of which are the main deterrents of cholera spread. While this strategy proved effective when instituted by the Nigerian government during the 2018 outbreak, it still requires increased government funding and outside investment to remain effective. Public health and safety continue to endure disadvantages, as the threat of cholera looms over the country.
GET INVOLVED:
For those looking to get involved in supporting the fight against cholera outbreaks in Nigeria, check out organizations such as WaterAid, Bread and Water for Africa, Save the Children and The Water Project, groups focused on supplying safe drinking water and sanitation to Nigeria, as well as many other countries in Africa. In addition, organizations like Doctors Without Borders, the World Health Organization, ICAP Global Health and Gavi, The Vaccine Alliance provide medical support to cholera patients in Nigeria and contribute to the development of disease control and prevention.

Julia Kelley
Julia is a recent graduate from UC San Diego majoring in Sociocultural Anthropology with a minor in Art History. She is passionate about cultural studies and social justice, and one day hopes to obtain a postgraduate degree expanding on these subjects. In her free time, she enjoys reading, traveling, and spending time with her friends and family.